
Vitamin D3: How to use the energy of the sun all year round
What will you learn in this guide?
- The vitamin D formation and absorption.
- The key function for the immune system.
- Too little sun = too little vitamin D
- How much vitamin D does a person need?
- Attention: No D3 without K2.
- The functions of K2.
- The differences in vitamin K2 form.
- Magnesium - an indispensable partner.
- Study shows: Liposomal vitamin D3 + K2 has higher bioavailability.
Vitamin D3 is essential for the human defense system to function normally. In case of a deficiency, our immune system is weakened and we run the risk of getting sick faster. That is why colds occur very often, especially in February and March, when vitamin D stores are depleted.
Other important functions of the vitamin are the maintenance of bones, teeth and muscle function. In addition, vitamin D contributes to the normal absorption and utilization of calcium and regulates the calcium level in the blood!
One thing quickly becomes clear: the body can’t do anything without the sun vitamin!
1. The Vitamin D formation and absorption
Vitamin D is actually not a vitamin at all, but a prohormone. This means that it is the precursor of a hormone that is first converted into an actively active hormone in the liver and kidneys as well as in various cells. This conversion always takes place by the organism, regardless of whether the vitamin D3 is produced with the help of sunlight or supplied via a dietary supplement.
Only a small part of vitamin D3, also known as cholecalciferol, is absorbed by the human body via vitamin D-containing animal products. The majority, around 80 to 90%, is produced by the human body on its own by converting cholesterol into vitamin D with the help of sunlight. The cholesterol is converted into vitamin D3 in the skin under the influence of UVB radiation [1,2].
2. The key function for the immune system
Research has shown that vitamin D serves as an important messenger in the control of the immune system. It influences both our innate and adaptive (acquired) immune systems. Each individual immune cell has vitamin D receptors on its surface and is able to convert vitamin D to the active form when needed.
Vitamin D regulates the immune system so that pathogens are fought early and no physical reaction, such as a cold, occurs in the first place [3]. Human T cells, which recognize and kill pathogens, are activated by the vitamin so that pathogens are blocked.
Thus, vitamin D supports the body's defenses, which protect humans from viruses and bacteria [4,5]. Defenses that protect against fungi or cancer cells, such as cathelicidin, are also supported by the vitamin in production [6,7,8].
For these reasons, vitamin D deficiency should be prevented at all costs, as otherwise autoreactive T cells are formed which attack the body's own cells and, in the worst case, even cause an autoimmune disease. Since vitamin D prevents the body from attacking itself because it cannot distinguish between its own and foreign cells, the vitamin is also known as an immunomodulator [9,10,11].
The support for infections
The importance of an adequate vitamin D supply has also been proven by numerous studies. An Italian research with 42 test persons showed that about 81% of the COVID-19 patients suffer from a vitamin D deficiency. Here, patients with acute vitamin D deficiency (below 10 ng/ml) had a 50% risk of death.
When the vitamin D level of SARS-CoV-2 infected individuals was above 10 ng/ml, the risk of death was only 5% and thus 10 times lower [12]. Various studies have also shown that an adequate supply of vitamin D has a positive effect on the course of influenza [13,14,15,16].
Here it is important to emphasize that vitamin D is not a cure for corona or other infectious diseases. However, a sufficient supply is a good prevention to protect the body.

3. Too little sun = Too little vitamin D
In Germany, about 60% of the population has a vitamin D deficiency. A D deficiency means that the body has less than 20 ng/ml of the vitamin in the blood serum [17]. Due to our geographic location and modern lifestyle, this is not surprising.
In order for vitamin D to form in the skin, it needs sunlight. Important to know: the wavelength of the light is of crucial importance. UV-B rays with a wavelength of 290 to 315 nm are needed for D production, which varies greatly depending on geographic location and especially on the time of year. Particularly in the dark season, vitamin D deficiency can therefore occur quickly.
The ozone layer in the stratosphere fulfills its protective function by not allowing high wavelengths of light 200 to 280 nm (UVC) and UV-B components above 290 nm to pass through. Of the UVB radiation of wavelengths above 290nm, only about 1% passes through the ozone layer, so we only have the opportunity to absorb 1%.
The challenge: especially for countries in the northern hemisphere, this 1% can only penetrate between 10 a.m. and 3 p.m., and only during the months of April to September. This is because it is only during this period that the angle from the earth to the sun is short enough for the light quanta to reach a UV index of 3. Anything below a UV index of 3 is not sufficient to produce vitamin D [18,19]. Also a challenge to vitamine D intake, most people are indoors at this time of day.
4. How much vitamin D does a person need?
There is no international guideline value for the daily requirement from the German Nutrition Society. Especially in the dark months, when the organism cannot produce the vitamin on its own, up to 5000 IU can be supplied daily. In order to find an optimal dosage for oneself, it is worthwhile to have a blood test to determine the appropriate, individual dosage under medical supervision. But even among doctors there are different opinions about which value is optimal. Too low a D level can demonstrably be detrimental to health. Now the question arises: what daily intake is healthy and sufficient?
Numerous sources define a D level between 40 and 60 ng/ml in blood serum as ideal. Values up to 60 ng/ml are considered safe in conventional, general medicine [20].
In order to benefit from the positive effects of the vitamin, experts recommend an equal-dose, permanent supply instead of a weekly or monthly overdosed cure. After all, our body does not produce extremely high doses at once in sunny weather, but rather the required amount every day in order to be protected.
Primitive people provide the answer:
Since the human organism is self-regulating, no overdose has ever been proven by the body's own production of a healthy person. For this reason, some physicians use primitive peoples, i.e. people who still live under pristine conditions, as a reference. Here it is to be investigated whether an overdose of the fat-soluble vitamin D3 is possible. In these people, who live at the height of the equator, a healthy vitamin D level of 50 to 90 ng/ml could be detected [21].
5. Attention: No D3 without K2
For vitamin D to work safely and reliably, D alone is not enough. As already mentioned above, vitamin D is significantly involved in the control of calcium absorption and is also responsible for the synthesis of some important proteins.
For these proteins to become active and exert their effect, vitamin K2 is important as a co-factor. Only in combination with K2 can the absorbed calcium be properly transported and utilized. Thus, two of the most important human proteins, the matrix GLA protein (MGP) and osteocalcin, have also been shown to be dependent on vitamin K2 [22,23,24,25].
The influence of vitamin K2
The protein osteocalcin is important for the formation of new bone. It ensures that the absorbed calcium is incorporated into the bones. Matrix GLA prevents calcium from accumulating in organs or vessels by binding the calcium and transporting it away [26].
If vitamin K2 is not present for this process, the proteins cannot act and there is a risk that the calcium will lead to calcification in the vessels and organs. Thus, kidney stones, arteriosclerosis, and numerous diseases, including myocardial infarction, are favored [27]. In addition, if calcium accumulates in the wrong places, it cannot fulfill its functions for bone health.
The right amount of K2
If vitamin D levels are high, vitamin K2 deficiency can quickly occur because K2 is also consumed for vitamin D activation. In this case, vitamin K2 can no longer be used for the other processes in the body described above [28].
Calcium in this case, even though the level in the blood is not too high, can be deposited on the vessels and organs due to the lack of vitamin K2 for utilization [29,30,31]. This is also partly the reason for the toxic effect of vitamin D in very high amounts.
Animal studies have shown that vitamin K2 deficiency can cause symptoms similar to those caused by a toxic, extremely high dose of vitamin D [32]. It is therefore not surprising that high vitamin D levels, which are normally good for bones, can increase the risk of bone fractures if vitamin K deficiency is also present [33].
Remember: When taking 1000 IU of vitamin D, always take at least 50 micrograms of vitamin K2 in parallel.
6. The functions of K2
In addition to its positive influence on bones, vessels and skin, vitamin K2 also has anti-inflammatory properties [36]. And the human brain also has an increased K2 concentration. Here, the vitamin contributes to the formation of protective compounds [37]. To simply explain the importance of the vitamin again: If a vitamin K2 deficiency occurs, there is a higher risk of dying from heart failure. This risk is as high as in people who smoke heavily and are also prone to heart failure [38,39].
Furthermore, the latest research shows that an adequate K2 supply should also be ensured in chronic kidney disease [40].

7. The differences in Vitamin K2 form
Vitamin K has different forms, but their effects are quite similar. The number designation is based on the number of chemical side arms which range from MK4 to MK13. The most widely studied forms are MK4 and MK7.
The MK7 form accumulates most effectively in the body, providing a sustained and adequate supply to all organs and tissues. By comparison, while MK7 remains available in the blood for more than 72 hours (half-life), the majority of MK4 is excreted after only about 1.5 hours. In addition, MK7 is significantly more effective than the MK4 form. Around 60 µg of MK7 show a better effect than a whole 500 µg of MK4 [41,42,43,44].
As with many molecules, there are two different forms of vitamin K2 MK7: the cis and trans form. These isomers have the same number of atoms, but a different spatial structure. Only the trans form of vitamin K2 MK7 can be utilized by the body. The cis form is ineffective for it! Unfortunately, many vitamin K2 products consist of up to 70 percent of the cis isomers.
A high-quality vitamin K2 dietary supplement should therefore always have the designation all-trans MK7!
8. Magnesium - an indispensable partner
What many people do not know: a magnesium deficiency can limit the effect of vitamins!
As already mentioned, vitamin D3 must first be converted by the body in order to work. The enzymes needed to do this, as well as the transport molecules that distribute vitamin D throughout the body, rely on magnesium. The parathyroid hormone (PTH) produced in the parathyroid gland, which regulates D conversion, also requires magnesium.
A high intake of vitamin D can therefore also lower magnesium levels, since significantly more is consumed for D activation. Regardless of whether vitamin D is taken from the sun or in the form of vitamin D supplementation, without magnesium, vitamin D can never develop its full effect and an overdose can even be harmful [46,47,48,49,50,51].
Since all known enzymes in vitamin D metabolism require magnesium, care should be taken to ensure an adequate supply.


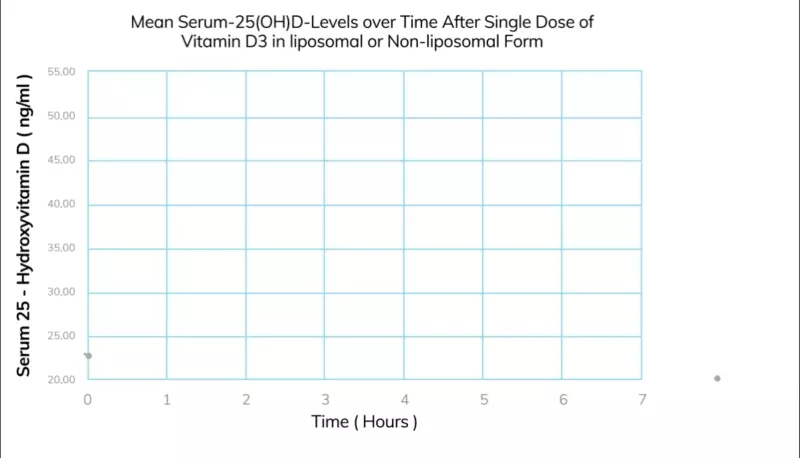
9. Study shows: Liposomal vitamin D3 + K2 has higher bioavailability
Recent research shows that vitamin D3 packaged in liposomes guarantees 13x higher absorption than conventional tablets. Since D is a fat-soluble vitamin, vitamin D intake can become a challenge.
Influencing factors such as the individual, human fat digestion or but the stomach contents can therefore lead to restrictions in vitamin D intake. The liposomal form ensures a consistent, unrestricted supply in daily intake.
The K2 used by ActiNovo is also the active MK7 all-trans form, which has a sufficient ratio of 75 µg all-trans MK7 K2 to 1000 IU = 25 micrograms vitamin D3! With the supplementation of the mineral magnesium, the vitamin D preparation can develop its full effect.
Read more now!


1) Gröber U. Vitamin D3 – ein altes Vitamin im neuen Licht. Med Monatsschr Pharm 2010;33(10):376 – 383.
2) Sylvia Christakos, Dare V. Ajibade, Puneet Dhawan, Adam J. Fechner, Leila J. Mady, Vitamin D: Metabolism, Rheumatic Disease Clinics of North America, Volume 38, Issue 1, February 2012, Pages 1-11, ISSN 0889-857X, http://dx.doi.org/10.1016/j.rdc.2012.03.00
3) Femke Baeke, Tatiana Takiishi, Hannelie Korf, Conny Gysemans, Chantal Mathieu, Vitamin D: modulator of the immune system, Current Opinion in Pharmacology, Volume 10, Issue 4, August 2010, Pages 482-496, ISSN 1471-489
4) Shuler FD, Hendrix J, Hodroge S, Short A (2013) Antibiotic-like actions of vitamin D. W V Med J 109:22–25 PMID: 23413544
5) Ramanathan B, Davis EG, Ross CR, Blecha F (2002) Cathelicidins: microbicidal activity, mechanisms of action, and roles in innate immunity. Microbes Infect 4:361–372 PMID: 11909747
6) Barlow PG, Svoboda P, Mackellar A, Nash AA, York IA, Pohl J, Davidson DJ, Donis RO (2011) Antiviral activity and increased host defense against influenza infection elicited by the human cathelicidin LL-37. PLoS ONE 6:e25333 PMCID: PMC3198734
7) Büchau AS, Morizane S, Trowbridge J, Schauber J, Kotol P, Bui JD, Gallo RL (2010) The Host Defense Peptide Cathelicidin Is Required for NK Cell-Mediated Suppression of Tumor Growth. J Immunol 184:369–378 PMCID: PMC2908520
8) Bruns H, Buttner M, Fabri M, et al (2015) Vitamin D-dependent induction of cathelicidin in human macrophages results in cytotoxicity against high-grade B cell lymphoma. Science Translational Medicine 7:282ra47-282ra47 DOI:10.1126/scitranslmed.aaa3230
9) Kamen, Diane L.; TANGPRICHA, Vin. Vitamin D and molecular actions on the immune system: modulation of innate and autoimmunity. Journal of molecular medicine, 2010, 88. Jg., Nr. 5, S. 441-450.
10) Maria C. Borges, Lígia A. Martini, Marcelo M. Rogero, Current perspectives on vitamin D, immune system, and chronic diseases, Nutrition, Volume 27, Issue 4, April 2011, Pages 399-404, ISSN 0899-9007
11) von Essen, Marina Rode, et al. Vitamin D controls T cell antigen receptor signaling and activation of human T cells. Nature immunology, 2010, 11. Jg., Nr. 4, S. 344-349.
12) Carpagnano, G.E.; Di Lecce, V.; Quaranta, V.N.; Zito, A.; Buonamico, E.; Palumbo, A.; Di Gioia, G.; Valerio, V.N.; Resta, O. Vitamin D deficiency as a predictor of poor prognosis in patients with acute respiratory failure due to COVID-19. J. Endocrinol. Investig. 2020.
13) Zhou, J.; Du, J.; Huang, L.; Wang, Y.; Shi, Y.; Lin, H. Preventive effects of vitamin D on seasonal influenza A in infants: A multicenter, randomized, open, controlled clinical trial. Pediatric Infect. Dis. J. 2018, 37, 749–754.
14) Sabetta, J.R.; DePetrillo, P.; Cipriani, R.J.; Smardin, J.; Burns, L.A.; Landry, M.L. Serum 25-hydroxyvitamin d and the incidence of acute viral respiratory tract infections in healthy adults. PLoS ONE 2010, 5, e11088.
15) Urashima, M.; Segawa, T.; Okazaki, M.; Kurihara, M.; Wada, Y.; Ida, H. Randomized trial of vitamin D supplementation to prevent seasonal influenza A in schoolchildren. Am. J. Clin. Nutr. 2010, 91, 1255–1260.
16) Arihiro, S.; Nakashima, A.; Matsuoka, M.; Suto, S.; Uchiyama, K.; Kato, T.; Mitobe, J.; Komoike, N.; Itagaki, M.; Miyakawa, Y. Randomized trial of vitamin D supplementation to prevent seasonal influenza and upper respiratory infection in patients with inflammatory bowel disease. Inflamm. Bowel Dis. 2019, 25, 1088–1095.
17) https://www.dge.de/presse/pm/neue-referenzwerte-fuer-vitamin-d/
18) 1. Caldwell M, Flint S. Stratospheric ozone reduction, solar UV-B radiation and terrestrial ecosystems. Clim Change. 1994; 28:375–94. doi: 10.1007/BF01104080.
19) Webb AR, Kline L, Holick MF. Influence of season and latitude on the cutaneous synthesis of vitamin D3: exposure to winter sunlight in Boston and Edmonton will not promote vitamin D3synthesis in human skin. J Clin Endocrinol Metab. 1988; 67:373–8
20) Power, M. L., & Dittus, W. P. (2017). Vitamin D status in wild toque macaques (Macaca sinica) in Sri Lanka. American Journal of Primatology, 79(6). doi:10.1002/ajp.22655
21) Uwe Gröber Die wichtigsten Nahrungsergänzungsmittel - Das Plus für Ihre Gesundheit Südwest, 2019, ISBN: 9783641233778
22) Vermeer C, Jie KS, Knapen MH (1995) Role of vitamin K in bone metabolism. Annu Rev Nutr 15:1–22 PMID: 8527213
23) Gallop PM, Lian JB, Hauschka PV (1980) Carboxylated calcium-binding proteins and vitamin K. N Engl J Med 302:1460–1466 PMID: 6990261
24) Hauschka PV, Lian JB, Cole DE, Gundberg CM (1989) Osteocalcin and matrix Gla protein: vitamin K-dependent proteins in bone. Physiol Rev 69:990–1047 PMID: 2664828
25) Inaba N, Sato T, Yamashita T (2015) Low-Dose Daily Intake of Vitamin K(2) (Menaquinone-7) Improves Osteocalcin γ-Carboxylation: A Double-Blind, Randomized Controlled Trials. J Nutr Sci Vitaminol 61:471–480 PMID: 26875489
26) Bügel S (2008) Vitamin K and bone health in adult humans. Vitam Horm 78:393–416 PMID: 18374202
27) Berkner KL, Runge KW (2004) The physiology of vitamin K nutriture and vitamin K-dependent protein function in atherosclerosis. Journal of Thrombosis and Haemostasis 2:2118–2132 DOI: 10.1111/j.1538-7836.2004.00968.x
28) Masterjohn C (2007) Vitamin D toxicity redefined: vitamin K and the molecular mechanism. Med Hypotheses 68:1026–1034 PMID: 17145139
29) El Asmar MS, Naoum JJ, Arbid EJ (2014) Vitamin K Dependent Proteins and the Role of Vitamin K2 in the Modulation of Vascular Calcification: A Review. Oman Med J 29:172–177 PMCID: PMC4052396
30) Theuwissen E, Smit E, Vermeer C (2012) The role of vitamin K in soft-tissue calcification. Adv Nutr 3:166–173 PMCID: PMC3648717
31) Cranenburg ECM, Vermeer C, Koos R, Boumans M-L, Hackeng TM, Bouwman FG, Kwaijtaal M, Brandenburg VM, Ketteler M, Schurgers LJ (2008) The circulating inactive form of matrix Gla Protein (ucMGP) as a biomarker for cardiovascular calcification. J Vasc Res 45:427–436 PMID: 18401181
32) Luo G, Ducy P, McKee MD, Pinero GJ, Loyer E, Behringer RR, Karsenty G (1997) Spontaneous calcification of arteries and cartilage in mice lacking matrix GLA protein. Nature 386:78–81 PMID: 9052783
33) Feskanich D, Weber P, Willett WC, Rockett H, Booth SL, Colditz GA (1999) Vitamin K intake and hip fractures in women: a prospective study. Am J Clin Nutr 69:74–79 PMID: 9925126
34) Cranenburg ECM, Schurgers LJ, Vermeer C (2007) Vitamin K: the coagulation vitamin that became omnipotent. Thromb Haemost 98:120–125 PMID: 17598002
35) Vermeer C (2012) Vitamin K: the effect on health beyond coagulation – an overview. Food Nutr Res. doi: 10.3402/fnr.v56i0.5329 PMCID: PMC3321262
36) Pan M-H, Maresz K, Lee P-S, Wu J-C, Ho C-T, Popko J, Mehta DS, Stohs SJ, Badmaev V (2016) Inhibition of TNF-α, IL-1α, and IL-1β by Pretreatment of Human Monocyte-Derived Macrophages with Menaquinone-7 and Cell Activation with TLR Agonists In Vitro. Journal of Medicinal Food 19:663–669 DOI: 10.1089/jmf.2016.0030
37) Carrié I, Portoukalian J, Vicaretti R, Rochford J, Potvin S, Ferland G (2004) Menaquinone-4 concentration is correlated with sphingolipid concentrations in rat brain. J Nutr 134:167–172 PMID: 14704312
38) Cundiff DK, Agutter PS (2016) Cardiovascular Disease Death Before Age 65 in 168 Countries Correlated Statistically with Biometrics, Socioeconomic Status, Tobacco, Gender, Exercise, Macronutrients, and Vitamin K. Cureus. doi: 10.7759/cureus.748 DOI: 10.7759/cureus.748
39) Gast GCM, de Roos NM, Sluijs I, Bots ML, Beulens JWJ, Geleijnse JM, Witteman JC, Grobbee DE, Peeters PHM, van der Schouw YT (2009) A high menaquinone intake reduces the incidence of coronary heart disease. Nutr Metab Cardiovasc Dis 19:504–510 PMID: 19179058
40) Westenfeld R, Krueger T, Schlieper G, et al (2012) Effect of vitamin K2 supplementation on functional vitamin K deficiency in hemodialysis patients: a randomized trial. Am J Kidney Dis 59:186–195 PMID: 22169620
41) Schurgers LJ, Teunissen KJF, Hamulyak K, Knapen MHJ, Vik H, Vermeer C (2007) Vitamin K-containing dietary supplements: comparison of synthetic vitamin K1 and natto-derived menaquinone-7. Blood 109:3279–3283 DOI: 10.1182/blood-2006-08-040709
42) Schurgers LJ, Knapen MHJ, Vermeer C (2007) Vitamin K2 improves bone strength in postmenopausal women. International Congress Series 1297:179–187 DOI: 10.1016/j.ics.2006.08.006
43) Sato T, Schurgers LJ, Uenishi K (2012) Comparison of menaquinone-4 and menaquinone-7 bioavailability in healthy women. Nutr J 11:93 PMCID: PMC3502319
44) Schurgers LJ, BV VPV, Thomas CP (2008) Vitamin K2 as MenaQ7™.
45) www.mri.bund.de/fileadmin/MRI/Institute/EV/NVSII_Abschlussbericht_Teil_2.pdf, S. 141
46) Zofková I , Kancheva RL. The relationship between magnesium and calciotropic hormones. Magnesium Research: Official Organ of the International Society for the Development of Research on Magnesium [1995, 8(1):77-84]
47) Risco F, Traba ML. Influence of magnesium on the in vitro synthesis of 24,25-dihydroxyvitamin D3 and 1 alpha, 25-dihydroxyvitamin D3. Magnes Res. 1992;5:5–14.
48) Risco F, Traba ML. Possible involvement of a magnesium dependent mitochondrial alkaline phosphatase in the regulation of the 25-hydroxyvitamin D3-1 alpha-and 25-hydroxyvitamin D3-24R-hydroxylases in LLC-PK1 cells. Magnes Res. 1994;7:169–178.
49) Rösler A, Rabinowitz D. Magnesium-induced reversal of vitamin-D resistance in hypoparathyroidism. Lancet. 1973 Apr 14;1(7807):803-4.
50) Zittermann, Armin. Magnesium deficit? overlooked cause of low vitamin D status?. BMC medicine, 2013, 11. Jg., Nr. 1, S. 229.
51) Rude RK, Adams JS, Ryzen E, Endres DB, Niimi H, Horst RL, Haddad JG Jr, Singer FR. Low serum concentrations of 1,25-dihydroxyvitamin D in human magnesium deficiency. J Clin Endocrinol Metab. 1985;61:933–940.